Brain plasticity
Brain plasticity
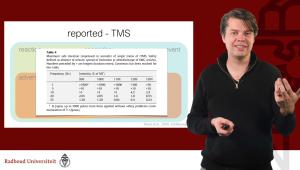
welcome to this lecture on the foundations of brain plasticity brain plasticity is perhaps one of the most important neurophysiological Concepts that we need to grasp to understand how we can translate from brain stimulation into clinical treatment it also is absolutely essential to understand the mechanisms of the most common non-invasive brain stimulation protocols that we use in cognitive neuroscience and when we're looking at the foundations I'm afraid that of course we'll have to go back to the neurons or specifically at the synapsis when we talk about plasticity we not mean the physical or structural changes of the brain and the shape that they have but often we refer to the strength of the synaptic information trend ER that the same signal coming in has either a stronger or a weaker consequence at what we call the postseptic neuron this is a beautiful drawing and I'm afraid that my drawings are a little bit more simplistic but it conveys the same idea we're going to look at an big pyramidal cell it has a dendritic tree at the top and it receives input from excitatory inter neurons if they fire Maybe because of a TMS pulse or because of ongoing brain activity they might transfer their signal across the sinapse and elicit an excitatory post synaptic potential a single one coming from one incoming neuron is completely irrelevant many neurons have tens of thousands of input coming and you can imagine that you don't want to be bothered where only one of those 10,000 is speaking to you so often we need a strong strong enough integrated post neptic potential where we converge the information from many incoming neurons to then elicit an action potential as an output it's an important function of a neuron to integrate information and to decide what is important and what isn't but not only the strength or the number of incoming signals is critical it's also when they arrive you can imagine that only when all these signals come together that they truly add up to an integrated excitatory potential and what we're learning is that neurons that right the this the one of a large set that comes a in a little bit earlier just before all the rest of its friends are firing that's a neuron that is predictive it gave you the information slightly earlier before the rest of the bulk was coming there are also neurons that are lagging a bit behind they might even deliver you input after you have already fired your action potential potential if you need to decide to which neuron you're going to listen better or more the next time around and which neurons you're going to ignore you're going to listen to those that had predictive information to those neurons that were arriving just before you got the main information before you delivered your action potential so the timing of the incoming signal relative to the timing of Your Action Potential is very important for a neuron to decide which imp is important and which can I ignore this principle is known as Spike timing dependent plasticity because you're going to increase the synaptic strength where the excitatory postseptic potential predicted your own action potential and you're going to decrease it where you were too late well you don't want to do this at random if a signal is coming in completely irrespective of and your own action potential not closed by either preceding or after you're not going to do anything with it at all you don't want to shut down your own brain when you're at rest now that means that the timing of the excitatory poptic potential relative to the action potential determents Spike timing dependent plasticity and we can um these mechanisms on what we're up or down regulating are often grouped together for the most well-known plastic it mechanisms long-term potentiation here in red uppr regulation or if they're just misfired in timing long-term depression this happens when we can specifically time our pulses but you might also realize that with ongoing spontaneous brain activity changing the threshold for how you're responding maybe how close or far away you are from your um action potential firing Baseline pardon me um will help to either increase the number of spontaneous firings that cross the threshold or actually decrease it this is a principle how we often think that plasticity inducing protocols might work specifically something like transcranial electric stimulation if we bring the neuron close through firing threshold something that was two week before now suddenly becomes an effective action potential you can imagine that there is a neuron trickling with some information it is coming on time but it is still too weak if you give this the extra boost it might lead to long-term potentiation or you might if you drive the resting Baseline in the other direction long-term depression these are neurophysiologically very complex mechanisms it's still under active investigation but when we're looking at into this we already know some of the core principles andd we're going to look at the cups and most of the signal being transferred is done by vesicles releasing for example a neurotransmitter this could be a glutamate an excitatory neurotransmitter and this is picked up by The receptors for long-term potentiation we are upregulating the number of our um receptors there is already nmda receptors that are picking up glutamate and then we have an extra facies an extra Reserve uh buffer of Empire receptors we can quickly Express on the syapse to very quickly listen better listen more to the same incoming signal long-term potentiation we can also remove them from the synaptic membrane the synaptic CFT and then we are not listening as hard long-term depression to evoke these protocols we've often and to study them we have often used uh animal models some of the most common ones are on the hippocampus in rodents actually you're looking now here at the hippoc cample slice in rodents and you can imagine the hippocampus is important for memory and for spatial navigation for structure learning all these kind of things that rely on learning from the environment about inducing plasticity the hypoc campus is fantastic and changing it synaptic weight very rapidly we also know the structure so if we're having one electrode on one exteral projection we can stimulate it elicits an action potential and we can record what is happening on the downstream ation right we can record that excitatory uh postseptic potential it matters on the specific protocol that we deliver if we deliver high frequency stimulation we we see an long-term potentiation and now with the same input suddenly the post neptic neuron responds stronger but if we deliver lower frequency or lower intensity stimulation this leads to a long-term depression okay I want to First rely on your intuition that it is a bit strange both of these are stimulation how can one lead to up and the other to down remember when we were talking about Spike timing dependent plasticity where we're saying that it matters how effective the stimulation is an ineffective stimulation means ah I'm going to ignore you for now long-term depression but an effective stimulation I'm going to listen to you better now if you want to dive a little bit deeper we're going to look at the signaling and and especially what is happening when we have glutamate driving on the syapse there is a whole signaling Cascade it's especially the calcium iron influx that is critical if calcium influx is very rapid that signals that we should have an upregulation of Empire receptors but if the flux of calcium is slow that leads to an reduction right there's a whole complexity on this up and down regulation and there are important structures like Cal modulin that are detecting this and changing it but often we are noting that there could be an is not a linear effect but there are more nonlinear effects such as here you see the inverted u-shape on the Ral flux and whether we see and potentiation or a depression and I want to uh conceptualize that a little bit more for you let's look at what is known as a a dose response curve or actually in this case a dose plasticity curve on the x-axis we have the total intensity of stimulation and on the y- axis the direction of change if you're healthy uh and I hope we all are then no stimulation also shouldn't elicit any change but very high intensity stimulation will lead to facilitation and the intermediate low intensity will lead to inhibition we can draw the do um plasticity curve through right you see that there's nothing changing if there's no input and we suddenly have to shift this curve can be different for every individual from one brain region to the other in fact the curve can change whether you're ill or whether you're healthy the curve can change at over your days the brain is highly adaptive it also highlights that the same stimulation protocol might have very different effects depending on the shape of this dose plasticity curve so how do we combine the idea of stimulation intensity with what we've learned about Spike timing depend plasticity here we see the conventional curve right depending on the timing we have inhibition or excitation if we look at low intensity stimulation all of your stimulation regardless of the timing is going to be ineffective to drive an action potential so now what we're left with is only the long-term depression side of that whole complex curve and if we de uh um stimulate at intermediate intensities we have to full curve but if we stimulate at high intensities then every input will drive an action potential and suddenly you can see that regardless of the timing we have long-term potentiation right this is why in some cases the timing is so important when we're thinking about the intermediate level but we can also drive it to the extremes I've highlighted Spike dang plasticity we've looked at the signups uh if you're interested in this topic there's a whole lot more to discover both about the cups but also the role for example that astrocytes those are not neurons they're gleo cells the role that they have in supporting synaptic plasticity and in some of the more recent developments in non-invasive brain stimulation consider for example ultrasound uh people are investigating how the estro sites are actually driving many of these synaptic effects but that's a topic for later discussion for now I want to remind you that although we can induce plastic effects it's probably an oversimplification to say that Protocols are the ones that are driving this effect we have ear discussed already earlier that the effect of a protocol is as much defend dependent on the parameters as it is on the state of the brain um we we're going to look at some of these uh protocols in the upcoming series uh upcoming slides for this talk remember an uh Theta burst protocol that has been proposed to be either inhibitory or excitatory depending on the structure of that uh stimulation but more recently we're seeing that it isn't as simple and that we might have con um intermittent Theta burst that is thought to be excitatory suddenly in many participants is inhibitory and it doesn't linearly increase if we deliver more stimulation in fact if we color code the different effects here inhibition in blue and excitation in red where every line every row is a participant and every column is a different stimulation protocol with more and more pulses either intermittent or continuous Thea burst we're seeing that it might might appear that it goes in all kinds of directions as as if there's nothing really consistent about it maybe we should rephrase this if we abandon the idea that excitation inhibition is solely due to the stimulation protocol but then what emerges is that many of these Protocols are consistent in inducing a plastic change regardless of the direction that isn't to say that there is no structure at all very systematic studies on stimulation protocols consider for example in transcanal electric stimulation have mapped out that the most robust and well known protocol here with with a conventional layout going for TW uh um 20 minutes at 1 milliamp has indeed you can see it here in the blue line an inhibitory effect but if either we increase the stimulation intensity to 2 milliamps or then also increase our stimulation duration an inhibitory protocol then suddenly becomes excitatory there is structure in the this it's just a whole lot more complex than any linear assumption and uh I was easy to ignore uh many of the protocols whether that were inhibitory or excitatory well if we look what happens in individual subjects right across the population there might seem as if there's no structure but if in for every participant We compare low frequency to high frequency stimulation we suddenly see that there's a very robust change within subjects we move from a more inhibitory to a more excitatory change even if overall we seem to be around zero there is a lot more to uncover in uh this topic and in this field in particular direction um that we we see that it's moving is not where we're only applying one stimulation protocol but where we're truly inducing a brain state ourselves now I want to unpack this slide for you we have an rtms protocol on the left that isn't particularly effective in inducing plasticity it seems um that's the middle line um but depending on the stimulation that precedes before the larger gray block we might suddenly have opposing effects if we have an cathodal stimulation we bring the brain State down and then this rtms protocol actually brings it back up it's a 5 Herz protocol it has an excitatory effect and it continues after the first measurement but if we do the reverse if we bring the brain state in the other direction with trans crano electric stimulation excitatory State then the same TMS intervention now has an inhibitory influence so depending on what happened before the same protocol has completely opposing effects and we see this in combinations of electric and magnetic stimulation or or or different electric stimulations on the right and that um interaction is known as homeostatic plasticity consider again an dose plasticity curve right this might be for one individual or for one brain region and with the arrow I'm pointing at a brain stimulation protocol of a certain intensity and there it has an inhibitory effect but if I would keep on stimulating again and again and again if it would continue to have an inhibitory effect that might shut down the whole brain circuit obviously that's not going to happen now instead what the brain does it shifts its curve and now the same stimulation protocol at the same intensity might actually have an excitatory effect this is the way how the brain helps to keep homeostasis to keep a healthy range and why the brain State matters on the effects of stimulation the complexity of plasticity is dependent on many different levels on our stimulation on the pharmacology on the circuits that we're uh going after and we see variability at all of these levels whenever you hear somebody talking about plasticity many of us are often shying away and this is too complex to tackle but we really need to start understanding this variability if we want to develop highly effective clinical interventions I hope that we're not too daunted by um the the future what lies ahead of us in today's lecture we have discussed some core foundations of plasticity we've looked at what happens at the syapse we've discussed Spike timing dependent plasticity where it matters when a stimulation is coming in the different relative timing of an input and an action potential we've also discussed how the plastic effects are depending on the total exposure the total maybe intensity we call it with primarily at lower intensities inhibitions and primarily excitory effects at higher intensities but then we were noticing that this isn't an general rule across everywhere we were seeing how this is dependent on the brain state that we can induce or on very specific parameters of the protocol and in the end we have discussed the complexities of variability of plasticity for now I want to thank you for your your attention
This lecture introduces the principles of plasticity including spike-timing-dependent, dose-dependent, and homeostatic plasticity, and discusses the neural underpinnings of plasticity. Finally, examples from the literature are used to demonstrate the use of NIBS for inducing neuroplastic changes. The goal of this lecture is to illustrate the interactions between NIBS protocols and neurophysiology that can lead to neuroplastic effects.
At the end of this lecture, students will be able to explain the principles underlying the neuroplastic effects of NIBS, and apply these principles for planning NIBS studies.
Topics covered in this lesson
- Introduction to principles of plasticity: spike-timing-dependent, dose-dependent, and homeostatic plasticity.
- Discussion on neural underpinnings of plasticity.
- Use of literature examples to demonstrate NIBS for inducing neuroplastic changes.
External links